

On-call arrangements continue to be an ongoing challenge for hospitals and healthcare systems. Ensuring continuity of coverage for not only emergency departments (ED) but for inpatient specialty practices has proven difficult for a variety of reasons. Many hospitals are required to maintain a panel of on-call physicians in order to preserve their trauma status and for regulatory compliance requirements.
However, the volume and acuity of ED coverage has increased across the country. Those changes, coupled with the declining supply of physicians and advanced care providers, combined with sustained focus on work-life balance, have resulted in continued upward pressure on on-call compensation in order to ensure proper coverage.
Emerging care models, including telehealth, hospital-at-home programs, and service-line consolidation, are also reshaping how organizations design and manage on-call coverage.
What should you consider when setting up on-call arrangements?
1. Structuring Coverage Arrangements
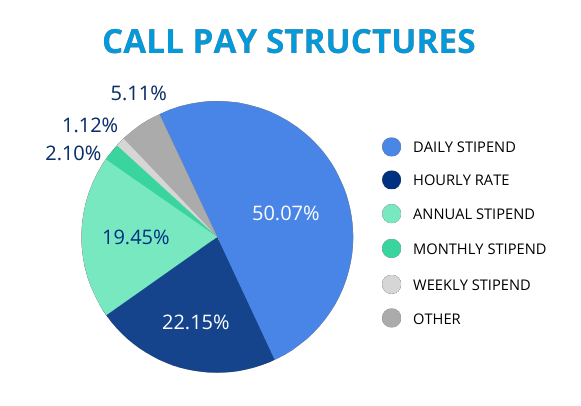
There are a number of ways to structure compensation within an on-call arrangement; as you can see in the chart below, a daily stipend is, without a doubt, the most common payment structure. Regardless of the compensation method, hospitals are finding more and more ways to compensate physicians for the burden of being on-call. We continue to see the percentage of physicians that receive payment for on-call services increase. According to Sullivan Cotter Provider On-Call Compensation Survey and MGMA On-Call Compensation Survey, an average of 50% to 70% of hospitals are now paying their physicians for on-call services.
2. Concurrent Coverage
Concurrent coverage comes in many shapes and sizes. The important thing to note when considering the utilization of a concurrent coverage model is that this coverage is provided by a single physician. This means a single physician is available to multiple facilities or multiple service lines.
As summarized in the chart below, there are many pros and cons to concurrent call coverage. One pro is the ability to cover multiple facilities or multiple specialties with a single call panel. This allows a hospital to maintain the needed coverage, even with limited physician supply and makes for easier tracking of the on-call panel. However, this can also be considered a con to providing concurrent coverage, because it requires a physician to be available to more than one facility or more than one specialty at any given time potentially increasing the burden and rate of pay for that coverage.
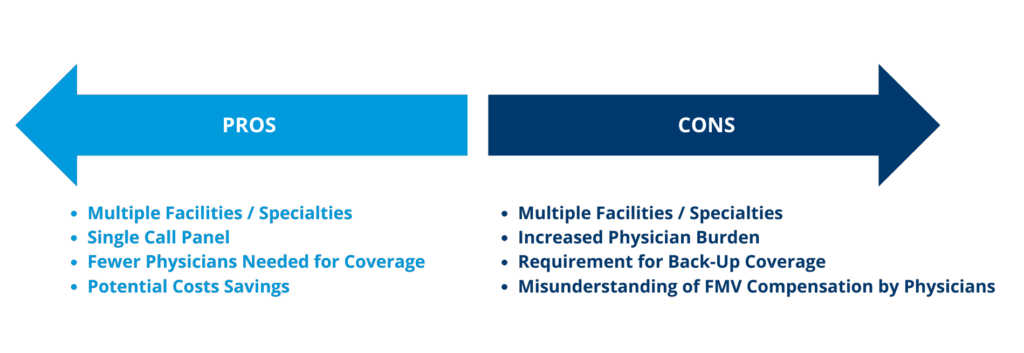
Because concurrent coverage can significantly increase physician burden and variability in workload, these arrangements often require additional scrutiny from a fair market value and compliance perspective.
On-Demand Webinar: Fair Market Value of On-Call Arrangements
Learn how hospitals are navigating call coverage design, concurrent coverage models, and FMV expectations.
3. Fair Market Value (FMV)
One compliance best practice is the evaluation of terms and compensation within a proposed arrangement in two ways. First, confirm that the arrangement meets a Stark exception and/or Anti-Kickback Statute safe harbor (as applicable) and second, confirm that compensation is FMV, commercially reasonable, and does not take into account the volume or value of referrals. In determining FMV for on-call arrangements, there are number of important components to consider:
- Physician Availability;
- Burden of Coverage;
- Acuity of Cases;
- Facility Designations; and
- Payor Mix
When evaluating on-call compensation, it’s important to distinguish between physician availability (being on-call), actual utilization (being called in or consulted), and case complexity. Each factor contributes differently to perceived burden and fair market value and should be evaluated independently.
Considering the burden of an on-call panel can take a few different forms, it’s important to include both the number of times the physician takes a phone call during an on-call shift and the number of times a physician is required to present on-site during an on-call shift. While a phone call doesn’t necessarily result in any type of face-to-face consultation or patient procedure, it does indicate how often the physician is interrupted during a call shift. On the other hand, the number of times that a physician presents on-site is a major indicator of the value of a call coverage panel. These factors, along with the acuity of cases, are indicators of what providers deal with while they are on-call.
Another important indicator of FMV is potential reimbursement for services provided when on-call. This has more of an impact for independent contractors than employed physicians due to billing and collection responsibilities. In considering reimbursement, it’s important to also consider the acuity of the cases as well as a facility’s payor mix. Reimbursement and the potential uncompensated care for self-pay patients or under-compensated care can have a potentially large impact on FMV and should be considered carefully.
In today’s environment, documenting the rationale behind on-call compensation—including coverage requirements, utilization data, acuity, and benchmarking support—is critical to demonstrating fair market value and commercial reasonableness.
As call coverage demands continue to evolve, organizations are increasingly reassessing existing arrangements to ensure compensation remains aligned with both market conditions and regulatory expectations.
LBMC helps you keep a PULSE on Fair Market Value (FMV)
LBMC helps healthcare organizations evaluate and document on-call arrangements through defensible FMV analysis, benchmarking, and ongoing compensation reviews. Our team works with hospitals and health systems to ensure arrangements remain compliant, commercially reasonable, and aligned with current market conditions.
Keeping a PULSE on FMV compensation can be complicated and time-consuming. Healthcare organizations are facing growing challenges. As a national leader in healthcare advisory services for over 30 years, our FMV calculators provide solutions for a variety of simple to complex provider compensation arrangements including: employment, call coverage and administrative services. And best of all, they’re fast and can be completed in less than a minute. If your healthcare organization is looking for an automated, web-based solution to assess compensation terms, the PulseFMV Calculator is your answer for defensible FMV support.
Content provided by LBMC Healthcare Compensation Valuation professional Jessica Webster.
On-Call Arrangements FAQs
What is the purpose of an on-call arrangement?
On-call arrangements ensure hospitals maintain continuous coverage for emergency departments and specialty services, helping meet patient care and regulatory requirements.
Why is fair market value important for on-call compensation?
Fair market value (FMV) ensures compensation is commercially reasonable and not tied to referral volume or value, which is critical for Stark Law and Anti-Kickback compliance.
What is concurrent call coverage?
Concurrent call coverage occurs when one physician provides coverage for multiple facilities or service lines at the same time, increasing both flexibility and potential workload.
What factors affect on-call compensation?
Key factors include physician availability, utilization, case complexity, acuity, facility designation, and payor mix.
How often should on-call arrangements be reviewed?
On-call arrangements should be reviewed regularly, especially when patient volume, service lines, or market compensation benchmarks change.
What documentation is needed for compliance?
Hospitals should maintain call schedules, utilization data, acuity metrics, compensation rationale, benchmarking support, and compliance review documentation.





